

The Kids Rock Difference, what they are, why we treat them, how we treat them, and FAQ.
The Kids Rock Difference
Here at Kids Rock We are going to strive in any way possible to make sure you and your child is comfortable during the procedure. We will be here to hold your hand, guide, and support you throughout this procedure from the pre- operative procedure, scheduling, phone calls, check in, and the day of the treatment. We promise to provide you the best care and treat your child the same way we would care for our own children. We look forward to meeting you!
What they are:
Frenectomies are essentially ties or bands of tissues that connect oral structures to the mouth. Every one has a combination of 7 that vary on severity. You have four in the back of you mouth that connects your cheeks to your gum tissues, two in front of your mouth that connects you lips to your gum tissues, and one under the tongue that connects your tongue to the floor of your mouth (tongue tied or ankyloglossia). Here at Kid Rock we are capable and willing to treat any of these seven tissue ties (Depending on your Child’s Individual Needs).
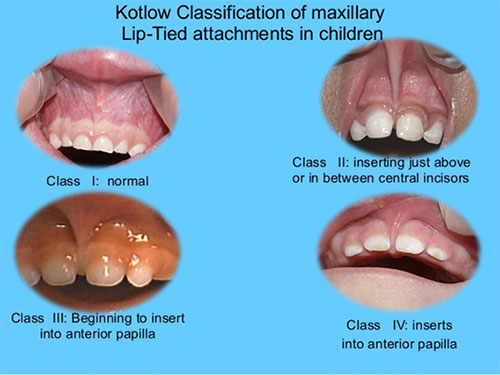
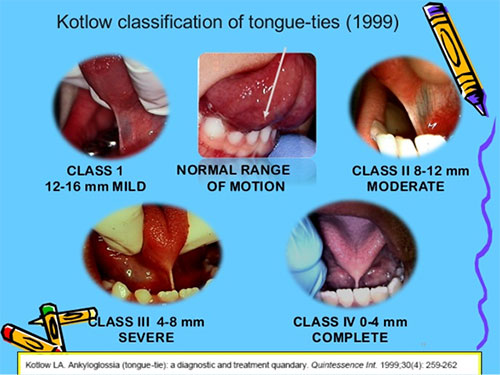
The most common types of frenectomies we treat are labial and lingual ties. For these types of ties, we classify them into different severity levels using Kotlow’s classification chart. This gives our provider and parents the most accurate description of severity.
For Lips: Class 1 is Normal, Class 2 Extends above the teeth but no further there is also no blanching (or whitening of the tissues when you lift it), Class 3 begins to extend between the teeth, and Class 4 Extends on to the palate.
For Tongues: Class 1 is a Mild Tie that still allows full range of motion (anywhere from 12-16mm in length), Class 2 moderate (anywhere from 8-12 mm in length), Class 3 or a severe tongue tie is 4-8mm in length limits the mobility of tongue making it difficult to touch the palate or clean teeth, and Class 4 is 0-4mm in length and essentially traps the tongue to the floor of the mouth. We only recommend treating Class 3 and 4 if signs and symptoms exist.
Why we treat them:
There are many reasons to treat oral ties. The most common reason why we treat them is for infants who may be struggling to nurse or who may be considered failure to thrive.
Lip Ties make it difficult for an infant’s lip to flare of the breast while nursing and tongue ties make it difficult for infant to swallow milks. Babies with more severe lip and tongue ties (class 3 and 4) will have increased Reflux/Colic, Gas, Thrush, Lack of Weight Gain, Choking on Milk, making Noises while Nursing, Excessive Drooling, and Difficulty Latching. Mother may be experiencing Crack/Bleeding/Blistered Nipples, Plugged Ducts, Discomfort while Nursing, Sleep Deprivation, Mastitis/Thrush, and a Compromised Milk Supply. If a mother or baby is experiencing any of these symptoms we recommend coming in for a consult.
In Toddler Lip Ties affect how well kiddos brush their front teeth making it harder or even more painful for the kid and the parent. It also creates a chipmunk affect by holding food or liquids closely to the front teeth. Both of these put kids at a very high caries risk. Decay on these front teeth usually leads to sedation on younger kids to have them repaired. Toddlers with Tongue Ties may have difficulty with pronunciation and struggle with talking and annunciating certain sounds. This may lead to kids needing speech therapy. They also cannot use their tongue to clean their palate or back teeth and this can lead to increased decay on the chewing surface of molars and incorrect development of the palate.
In Older Kids/Teenager/Adults Lip ties can create a diastema (space between the two front teeth) which is usually closed during ortho and may need to be correct before active ortho can end. Tongue ties can still continue to cause speech impediment but is can also lead to child need an expanded to open the palate. When you swallow without a tongue tie your tongue puts pressure the palate and develops the shape without continuous pressure the palate may not develop fully (leading to the need of an expander from an orthodontist). Lower lip ties at this age range if tight enough can cause recession of the lower central incisors putting the patient at risk of needing to see a periodontist at younger age or losing these teeth all together.
How we treat them:
If you choose to go to an ENT (Ear Nose and Throat Doctor) to have a frenectomy revised then your child will need to go under General Anesthesia to have the procedure done and it may be completed with a scalpel or surgical scissors. One of the benefits of having the procedure done at a Kids Rock instead of an ENT office is instead of having your kid put under General Anesthesia we can complete the procedure here in office with the patient awake and with a diode laser. We do not promise same day treatment but try and accommodate patients as quickly and efficiently as possible.
The first visit is the consult. At this visit we do not pressure parents we just diagnose the classification of lip and tongue tie then we give you your options and prepare you for what to expect on the day of the procedure.
Important things to remember Pre- Operative:
- We use anesthetic to numb the area (ensures patient doesn’t feel discomfort)
- We use a diode laser (heals more efficiently and decreases hemostasis)
- Parents aren’t allowed in the room during the procedure (for laser safety)
- We wrap patient of certain age for their safety
- We use Nitrous (Helps patient relax)
- You will need to do stretches after the procedure to ensure it heals properly
After the family gets scheduled and is able to return for the actual procedure, we always have the parent come in the room with the patient and answer any questions and cover post-operative instruction we then get the patient sat in the chair or wrapped and then walk the parents out. The doctor then comes in and completes the procedure this takes approximately 5-10 minutes to do. We then welcome the family back in the room. Older patients get a popsicle to help with the feeling of anesthetic or mothers are allowed to nurse and have the room for as long as you need.
Important things to remember Post- Operative:
- Anesthetic takes approximately 1-4 hours to end during this time be careful your child does not bite themselves.
- It may be sore and painful once anesthetic wears office previous patient compare this to the feeling of burn or canker sore in the mouth.
- It’s normal for children to be fussy after the procedure.
- Start with a cold and soft diet then work your way back to solid food. (Avoid Spicy and Acidic Food)
- Take Tylenol and Motrin on a 4-hour rotation to reduce post-operative sensitivity
- Ensure patient keep there hands out of there mouth
- Infection is a low encounter with this procedure
- Low grade fever is normal to encounter.
- Color change is normal (red, white, orange, yellow)
- Do the stretches 4-5 times a day for the next 4-6 weeks
- You may need to follow up with a lactation consultant or a speech therapist
- You can come in anytime after the procedure to follow up with the provider in regards to healing
FAQ (Frequently Asked Questions):
- What is the youngest you’ll treat?
- We feel confident in helping children as young as a day old.
- What is the oldest you’ll treat?
- There is no age to old to have the procedure done. As long as you feel comfortable completing the stretches for the patient, we can complete the procedure.
- How long does it take to heal?
- 4-6 weeks to completely heel.
- What are the chances of it reattaching incorrectly?
- If stretches are done frequently and correctly there is a very low chance of the tissue reattaching. If stretches are not being completed then there is a very high chance of it reattaching.
- Can this cause permanent damage to my child?
- Very low chance of any damage occurring to your child the laser is a diode and cuts slowly. That is also why we take precautions like using the wrap to keep your child safe from harm.
- Do I have to leave the room during treatment?
- Yes, this is our office policy and is required for parents to leave before this procedure will start.
- What Speech therapist do you recommend?
- Sprout Speech Therapy, LLC (719) 999-8417
- How Quickly will my child’s speech improve?
- Every child is different and parents have noticed and immediate difference in their child’s speech. But it does take work and practice on the child behalf to learn new sounds and that is why we recommend help from a speech therapist.
- What Lactation consultant do you recommend?
- Pikes Peak Lactation (719) 321-6143
- Will Nursing Improve Immediately?
- Every child is different and parents have noticed and immediate difference in their child’s nursing but we do recommend following up a lactation consultant.
- Will you put my kid under general anesthesia to treat a frenectomy?
- We can use a type of sedation to complete the procedure general/oral sedation but usually our providers complete the procedure with the patient awake.
- Will you do the procedure with the scissors instead of the laser?
- No, we only use a diode laser.
- Do you use a CO2 or Water Laser?
- No, we only use a diode laser.
- Do you have to wrap my child to complete the procedure?
- Yes, if the child is under that age of 4 and cannot complete the procedure by just laying the chair. We do this to make sure your child is safe. If we cannot do the procedure safely then we won’t do it. We do not wrap older children who can tolerate the procedure.
- Will it get infected?
- No infection is not common with these procedures. Ensure you are brushing like normal to help keep the area clean
- Is Swelling Normal?
- Yes, Swelling is normal. Cold foods will help reduce swelling and all swelling should go away within the next 1-3 days. The swelling should not close the air way and make it hard for your child to breath. Swelling may increase if your child bites themself.
- How Long Does It Take?
- The procedure takes from 5-10 minutes.
- What is the Link to the Post-Operative Video I watched in Office?
- https://www.youtube.com/watch?v=jCQ6xBAbbhA
- When do I start the stretches?
- We recommended starting the stretches withing the first 1-2 hours after the procedure since your child will still be numb the discomfort should be minimal.
- When can I brush my child’s teeth?
- That night following the procedure you’ll be allowed to start brushing your kid’s teeth. Just remember the area may be sensitive.
- Can my child use their pacifier?
- Yes, your child can still use a pacifier.
- Is it normal for my child to struggle when I do the stretches?
- Yes, Kids especially young kids may not like it when you do the stretches this can be due to post-operative sensitivity but it can also be due to the lack of control they are facing.
- Can I use Orgel or Vitamin E oil on the surgical site?
- You can use Orgel (at a certain age) or Vitamin E oil to elevate discomfort or promote healing. This is not Doctor recommended and is based on your personal preference.